Cheatsheet 4
This document was uploaded by user and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this DMCA report form. Report DMCA
Overview
Download & View Cheatsheet 4 as PDF for free.
More details
- Words: 594
- Pages: 1
Loading documents preview...
Respiratory Therapy Cave Respiratorytherapycave.blogspot.com Neonatal and Pediatric Guidelines and Calculators
Determining Neo and Peds ETT, laryngoscope, and Ideal Tidal Volume: Laryngo Cm @ Cm @ Min Age Weight ETT Max scope (kg) lipline Nasal VT VT Premature Premature Term 3 months 6 months 1 years 2 years 3 years 4 years 5 years 6–7 years 8 – 10 years
0.5 – 1 1. – 2 3.0 5.5 7 10 12 14 16 18 20 22 25
10 – 12 years 12 – 14 years
30 35 35 40 40 45
30
2.5 2.5 – 3.0 3.0 – 3.5 3.5 – 4.0 3.5 – 4.0 4.0 – 4.5 4.5 – 5.0 5.0 5.5 5.5 6.0
Straight Straight Straight Straight Straight Straight Straight any any Any Any
6.0 – 6.5
3-6 7–8 9 – 10 10 11 12 13 15
9
27.5 35 50 60 70 80 90 100 110 125
38.5 49 70 84 98 102 116 130
150
210
22 - 24 150 175 175 200 200 225
210 245 245 280 280 315
14 17 19
18
Any
6.5
Any
7.0
Any Any Any
Neo VT chart Neo VT chart Neo VT chart
175
1) ETT Size in ID (mm) = 4*(Age/4) 2) Depth oral = Age+13 or 3*ETT size/2 or 6+wt(kg) 3). Tidal Volumes based on pediatric guidelines of 5-7cc/kg ideal body weight 4) For neonates, the NRP suggested guideline for securing the ETT is weight in kg = 6 (2kg+6 = 9cm at lip)
Normal Pediatric Respiratory Rate and Heart Rate Kg Asleep Awake HR RR RR 0-1 day 30-40 94-145 1-7 day 30-40 120-160 8-30 day 30-40 115-190 Infant to =<4 30-40 40-70 120-130 1 month Infant to =<7 22-30 55-75 130 6 month 1 year =<10 16-24 25-42 120 2-3 years 12-14 14-26 20-36 115-125 4-5 years 16-18 16-20 18-32 100-110 6-8 years 20-26 12-16 16-30 90-100 10-12 32-42 12-25 75-85 >14years >50 12-18 70-100 respiratorytherapycave.blogspot.com 09/07/2009
Severe Distress
RR>60 RR>50 RR>40 RR>40 RR>35 RR>30
Setting up CPAP for a neonate: 1. 5–6 CWP good place to start 2. 7 – 8 CWP if FiO2 needs >60%, or signs increased SOB 3. If SpO2 > target range, down FiO2 by 5–20, then allow 4 minutes for stabilization between each change. 4. If SpO2 < target range, up FiO2 by 5–20, then wait 4 min for stabilizing between changes 5. Continue assuring AW patent, HR > 100, & infant not apneic. Suspected PPHN: - Target SpO2 = 96 – 99% - Do pre and post-ductal SpO2s - Pre-ductal: SpO2 = right arm ABG = R. Radial - Post-ductal: SpO2 = feet ABG = umb.artery - If PO2 difference >15mmHg= R to L shunt of Ductus ateriosis Suspected cyanotic heart disease: - Consider 100% O2 challenge - If no response in pt. with no respiratory distress, transfer pt.
Guidelines for Set-up of ventilator for Pediatrics: 1. Pt Range: Pediatric (if ideal VT > 40cc<400) 2. Mode: PC if < 10kg, otherwise PRVC 3. VT: 5-7 cc/kg post-term to 14 YO 4. PIP: Not > 30 5. PEEP: Start 4 – 5 CWP 6. FiO2: 5 – 10% above pre-intubation adjust to maintain desired SpO2. 7. Rate: Normal for age 8. I-time: a. Maintain I:E of 1:2 9. I-Rise time: As appropriate for patient to create pseudo sign wave. 10. PIP limit: 2-3 >PIP (other alarms as appropriate) Higher PIP & VT may be needed in certain cases. Consult physician if unable to ventilate at recommended settings. Settings may also be unique to your particular ventilator, or protocols at your particular hospital.
Determining Neo and Peds ETT, laryngoscope, and Ideal Tidal Volume: Laryngo Cm @ Cm @ Min Age Weight ETT Max scope (kg) lipline Nasal VT VT Premature Premature Term 3 months 6 months 1 years 2 years 3 years 4 years 5 years 6–7 years 8 – 10 years
0.5 – 1 1. – 2 3.0 5.5 7 10 12 14 16 18 20 22 25
10 – 12 years 12 – 14 years
30 35 35 40 40 45
30
2.5 2.5 – 3.0 3.0 – 3.5 3.5 – 4.0 3.5 – 4.0 4.0 – 4.5 4.5 – 5.0 5.0 5.5 5.5 6.0
Straight Straight Straight Straight Straight Straight Straight any any Any Any
6.0 – 6.5
3-6 7–8 9 – 10 10 11 12 13 15
9
27.5 35 50 60 70 80 90 100 110 125
38.5 49 70 84 98 102 116 130
150
210
22 - 24 150 175 175 200 200 225
210 245 245 280 280 315
14 17 19
18
Any
6.5
Any
7.0
Any Any Any
Neo VT chart Neo VT chart Neo VT chart
175
1) ETT Size in ID (mm) = 4*(Age/4) 2) Depth oral = Age+13 or 3*ETT size/2 or 6+wt(kg) 3). Tidal Volumes based on pediatric guidelines of 5-7cc/kg ideal body weight 4) For neonates, the NRP suggested guideline for securing the ETT is weight in kg = 6 (2kg+6 = 9cm at lip)
Normal Pediatric Respiratory Rate and Heart Rate Kg Asleep Awake HR RR RR 0-1 day 30-40 94-145 1-7 day 30-40 120-160 8-30 day 30-40 115-190 Infant to =<4 30-40 40-70 120-130 1 month Infant to =<7 22-30 55-75 130 6 month 1 year =<10 16-24 25-42 120 2-3 years 12-14 14-26 20-36 115-125 4-5 years 16-18 16-20 18-32 100-110 6-8 years 20-26 12-16 16-30 90-100 10-12 32-42 12-25 75-85 >14years >50 12-18 70-100 respiratorytherapycave.blogspot.com 09/07/2009
Severe Distress
RR>60 RR>50 RR>40 RR>40 RR>35 RR>30
Setting up CPAP for a neonate: 1. 5–6 CWP good place to start 2. 7 – 8 CWP if FiO2 needs >60%, or signs increased SOB 3. If SpO2 > target range, down FiO2 by 5–20, then allow 4 minutes for stabilization between each change. 4. If SpO2 < target range, up FiO2 by 5–20, then wait 4 min for stabilizing between changes 5. Continue assuring AW patent, HR > 100, & infant not apneic. Suspected PPHN: - Target SpO2 = 96 – 99% - Do pre and post-ductal SpO2s - Pre-ductal: SpO2 = right arm ABG = R. Radial - Post-ductal: SpO2 = feet ABG = umb.artery - If PO2 difference >15mmHg= R to L shunt of Ductus ateriosis Suspected cyanotic heart disease: - Consider 100% O2 challenge - If no response in pt. with no respiratory distress, transfer pt.
Guidelines for Set-up of ventilator for Pediatrics: 1. Pt Range: Pediatric (if ideal VT > 40cc<400) 2. Mode: PC if < 10kg, otherwise PRVC 3. VT: 5-7 cc/kg post-term to 14 YO 4. PIP: Not > 30 5. PEEP: Start 4 – 5 CWP 6. FiO2: 5 – 10% above pre-intubation adjust to maintain desired SpO2. 7. Rate: Normal for age 8. I-time: a. Maintain I:E of 1:2 9. I-Rise time: As appropriate for patient to create pseudo sign wave. 10. PIP limit: 2-3 >PIP (other alarms as appropriate) Higher PIP & VT may be needed in certain cases. Consult physician if unable to ventilate at recommended settings. Settings may also be unique to your particular ventilator, or protocols at your particular hospital.
Related Documents

Cheatsheet 4
February 2021 0
Dcs Cheatsheet
February 2021 1
Postgresql-cheatsheet
February 2021 0
Seo-cheatsheet
February 2021 5
Fretboard Cheatsheet Workbook
February 2021 1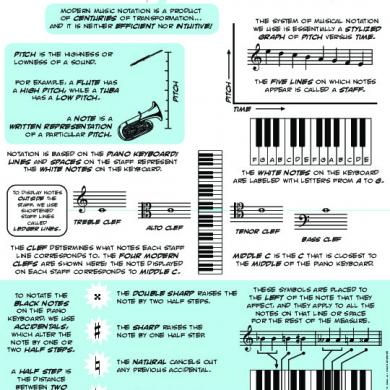
Music Theory Cheatsheet
February 2021 0More Documents from "Manas George"
Cheatsheet 4
February 2021 0
Neonatal Resuscitation Program
February 2021 1

100 Great: Italian
January 2021 0
The Sixth Book Of Moses
March 2021 0